

Abstract
Objectives: The aim of this study was to provide a randomized controlled trial comparing the outcomes of different access sizes used in the solo ultrasonic-guided minimally invasive percutaneous nephrolithotomy (mini-PCNL). Methods: From January 2018 to December 2019, a total of 160 cases with single renal stones of <25 mm were randomized to undergo mini-PCNLs with Fr16, Fr18, Fr20, or Fr22 accesses. All accesses were established with the axis of the target calyx as the marker for puncture location and then expanded to the desired size. Hemoglobin reduction, operative time, stone-free rate, complications, etc., were all recorded and assessed. Results: The demographic data were similar, and there were no significantly intergroup differences in stone-free rate, complications, and hospital stay time. The hemoglobin reduction was comparable and was 0.9 ± 0.6, 0.9 ± 0.7, 1.0 ± 0.5, and 1.1 ± 0.7 g/dL for the groups Fr16, Fr18, Fr20, and Fr22, respectively. The operative time was 53.4 ± 14.5, 48.5 ± 15.2, 42.8 ± 13.3, and 43.3 ± 13.1 min for the 4 groups, which decreased significantly from group Fr16 to Fr20, but there was no significant difference between Fr20 and Fr22 groups. Conclusions: The axis of target calyx is a reliable marker for establishment of percutaneous renal access under ultrasonic guidance. The surgical outcomes of different access sizes were comparable, but the operation time was significantly shortened with the increase of size. However, Fr22 was not more efficient than Fr20.
Introduction
Percutaneous nephrolithotomy (PCNL) remains the standard procedure for larger than 2-cm kidney stone and is eligible for other kinds of stones located in the kidney and upper ureter which are unfavorable for shock wave lithotripsy or retrograde lithotripsies. Despite considerable advances in the technology and equipment of PCNL, nearly one-fourth of patients still experience postoperative complications, among which bleeding is still the most important concern [1, 2]. Multiple causes have been associated with PCNL-related bleeding, of which the direction and size of the renal access have been identified as the 2 most important factors [3]. In previous studies, we proposed based on animal experiments and clinical practice that the access passing through the axis of the target renal calyx can minimize the damage to the blood vessels in the renal parenchyma [4, 5]. In addition to the path of the renal access, the size of the renal access is directly related to the damage of renal parenchyma and the efficiency of stone clearance. Previous studies have shown that the access of standard PCNL from Fr22 to Fr30 has no significant relationship with stone removal efficiency, but larger accesses are significantly more associated with bleeding [6, 7].
In recent years, miniaturization of PCNL has been a development trend. Today, the increasingly minimally invasive PCNL (mini-PCNL) through the accesses from Fr16 to Fr22 has been taken as a reasonable alternative to the standard PCNL [8, 9]. Compared with standard PCNL, the miniaturized accesses of mini-PCNL reduced the damage to renal parenchyma and also decreased the efficiency of stone clearance [10]. The available literature shows that the morbidity of mini-PCNL is less, and the stone-free rate is equal to that of standard PCNL; however, as the size of the access decreases, more time is needed to clear the fragments [11]. As for the Fr16 to Fr22 accesses that are commonly used in the mini-PCNL, whether the difference in the access size will be the same has not been fully clarified. Therefore, further assessment of the access size-related outcomes for mini-PCNL is needed. The aims of this study were to illustrate the renal access size-related outcomes through comparing the Fr16, Fr18, Fr20, and Fr22 mini-PCNLs for the single, maximum diameter <25 mm renal stone.
Methods
A total of 160 patients who required mini-PCNL surgery with the single, maximal stone diameter <25 mm at our institute were enrolled in a single-center prospective randomized controlled trial between January 2018 and December 2019. For details, please see the CONSORT 2010 checklist, in supplementary materials. The cases were equally randomized into 4 groups (40 patients in each study arm) and named group Fr16, group Fr18, group Fr20, and group Fr22 according to the renal access size used during the mini-PCNL procedures, respectively. All subjects have given their written informed consent, and the study protocol was approved by the institute’s committee on human research. The trial was approved by the local ethics and research scientific committee. A written consent was taken by all the patients after explaining the details of the procedure. Sealed envelopes equally nominating one of the 4 access sizes were used for the randomization process. All the procedures were done by 2 experienced urologists in the field of endourology, and none of them was in the learning curve. Exclusion criteria were age <18 years, anomalous kidney, any bleeding disorder and severe cardiopulmonary disease, and the delayed or 2-stage PCNL whose accesses had been built before. Patients with positive urine culture were treated with appropriate antibiotics before the mini-PCNL. Demographic characteristics, size of the stone, degree of hydronephrosis, hemoglobin drop, stone-free rate, transfusion rate, complication(s), hospital stay, and nephrostomy removal time were recorded and analyzed for all the groups.
The procedures were performed on an inpatient basis under general anesthesia with the use of solo ultrasonic-guided PCNL technique described before [4]. In summary, an Fr6 ureteral catcher was inserted with the patient in the lithotomy position, and then the patient was positioned in the prone position with renal area padding. Normal saline was retrogradely and continuously infused via the indwelling ureteral catheter from an infusion bag. Ultrasound was performed to find the desired calyx, and then an 18-gauge needle was inserted from the selected skin point to the axis of the target calyx under real-time ultrasound monitoring (Fig. 1). Following the insertion of a guide wire into the renal pelvis, the tract was dilated over the wire up to 16, 18, 20, or 22 Fr using a sequential fascial dilator. The mininephroscope and holmium laser were used to break stones, and the fragments were removed by rinsing through the peel-away sheath. At the end of the surgery, an indwelling double-J stent and nephrostomy tube were routinely placed.

The target calyx axis was used as the ultrasonic-guided marker to achieve percutaneous renal puncture. Schematic diagram in the left presents the needle entering the collecting system from the axis of the calyx along the ultrasonic guide line. Schematic diagram in the right displays the axis of the desired calyx on an ultrasonic image, and the ultrasonic guide line can assist the puncture needle to enter the collecting system from the axis of the desired calyx.
The target calyx axis was used as the ultrasonic-guided marker to achieve percutaneous renal puncture. Schematic diagram in the left presents the needle entering the collecting system from the axis of the calyx along the ultrasonic guide line. Schematic diagram in the right displays the axis of the desired calyx on an ultrasonic image, and the ultrasonic guide line can assist the puncture needle to enter the collecting system from the axis of the desired calyx.
The primary outcomes were the operative time and hemoglobin reduction. The operative time was defined as the time from the indwell of the ureteral catcher to the double-J stent confirmed in the right position. Serum levels of the hemoglobin were measured preoperatively and overnight after the procedure in a single laboratory. Stone-free rate, complications, nephrostomy time, and hospital stay seemed as the secondary outcomes. CT was performed on the third or fourth postoperative day to assess the stone-free status according to the patient’s postoperative recovery status. The stone fragments no >2 mm were considered as stone free, and then the nephrostomy tube was removed. The double-J stent was removed 2 weeks later in the daytime ward.
The calculation of the sample size was done using PASS 11 indicating 95% as confidence level and a confidence interval (margin of error) of 15%. The mean (±standard deviation) and frequency (percentage) values were used to express data. Statistical analysis was performed by using SPSS 18.0 software using the χ2 test for categorical variables and variance analysis for continuous variables. The level of significance was defined as p < 0.05.
Results
A total of 160 patients were equally randomized into 4 groups, and all procedures succeeded (Table 1). One patient in group Fr16 and 2 patients from group Fr22 were not included in the final analysis for the multiple accesses used. The preoperative assessment revealed resembling characteristics among the 4 groups. There were a greater number of patients with a history of open surgery in groups Fr20 and Fr22 (10.0 and 13.2%) when compared to groups Fr16 and Fr18 (5.1 and 5.0%), although this difference was not statistically significant (p = 0.489).
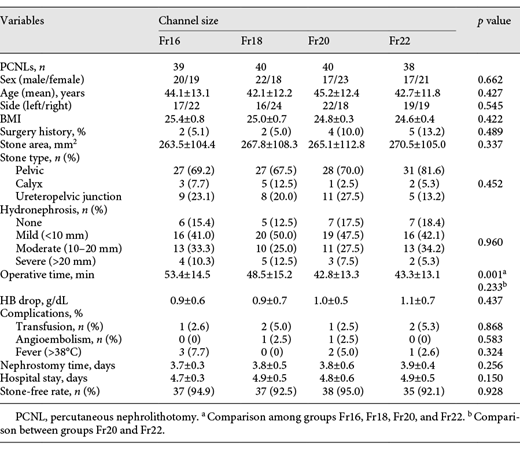
Mean operative time was 53.4 ± 14.5, 48.5 ± 15.2, 42.8 ± 13.3, and 43.3 ± 13.1 min for Fr16, Fr18, Fr20, and Fr22 groups, respectively (p = 0.001). Statistical analysis showed that the operative time significantly decreased from group Fr16 to Fr20, but it was similar in groups Fr20 and Fr22. There was no difference in blood transfusion rate (2.6 vs. 5.0 vs. 2.5 vs. 5.3%, p = 0.868), angioembolization rate (0 vs. 2.5 vs. 2.5 vs. 0%, p = 0.583), and postoperative fever (managed without additional antibiotics, 7.7 vs. 0 vs. 5.0 vs. 2.6%, p = 0.324). One patient each in groups Fr16 and Fr20 and 2 each in groups Fr18 and Fr20 received blood transfusion, of which 1 patient in group Fr18 and 1 patient in group Fr20 required angioembolization. However, hemoglobin reduction was not significantly different among the 4 groups (0.9 ± 0.6, 0.9 ± 0.7, 1.0 ± 0.5, and 1.1 ± 0.7 g/dL, respectively, p = 0.437). The nephrostomy drainage and hospital stay time showed no significant differences among the 4 groups. Stone-free rates were comparable among groups and were 94.9, 92.5, 95.0, and 92.1%, respectively (p = 0.928).
Discussion
Puncture and dilatation through renal parenchyma to the collecting system were the requisite procedures to build renal access for PCNL. The procedures of puncture and dilatation were also the most likely factors to cause injury to renal vessels, which have been considered as the key determinant of the PCNL-related bleeding [12]. Based on the anatomical background, the renal artery divides into 2 branches to give out segmental artery after entering the renal hilum and then divides into interlobar arteries to travel through the renal column. At the bottom of renal pyramid, the arcuate arteries arise from the interlobar arteries and give subbranches (interlobular arteries) into the cortex (Fig. 2) [13]. Therefore, the renal column is rich in blood vessels, while the renal pyramid is a relative hypovascular area. If we consider a renal pyramid to be a cone, the center line of the renal pyramid is the farthest path from the surrounding interlobar arteries. In other words, puncture from the center line of the renal pyramid to the corresponding calyx can minimize the damage to renal vascular. However, it is very difficult for us to conduct puncture through the central line of the renal pyramid under the ultrasonic guidance because the renal pyramid is hard to be identified by ultrasonic scanning. Fortunately, the calyx which presents as a hypoechoic image under ultrasonic scanning is easy to be recognized. According to the principle of one-to-one correspondence between the renal pyramid and the calyx, extension of the center line of the renal pyramid will coincide with the axis of the corresponding renal calyx. Therefore, the axis of calyx could be used as a safe marker for puncture under the ultrasonic guidance.

The relationship between vascular distribution and puncture route during PCNL. The diagram in the left is a cross-section of the kidney to illustrate the puncture through the axis of calyx can avoid renal vascular damage. The diagram in the right is a local enlargement of the renal pyramid and its peripheral vascular distribution, which shows the corresponding relationship between the renal pyramid and the calyx, and the puncture path through the axis of the calyx will minimize the damage to the vessels around the renal pyramid.
The relationship between vascular distribution and puncture route during PCNL. The diagram in the left is a cross-section of the kidney to illustrate the puncture through the axis of calyx can avoid renal vascular damage. The diagram in the right is a local enlargement of the renal pyramid and its peripheral vascular distribution, which shows the corresponding relationship between the renal pyramid and the calyx, and the puncture path through the axis of the calyx will minimize the damage to the vessels around the renal pyramid.
In theory, when the hypoechoic image of the calyx reaches its maximum cross-section under the ultrasonic scanning, the midline of the image is the axis of the corresponding calyx. Based on our experience, it is not always possible to accurately enter the collection system from the axis of the desired calyx. However, it is still a relatively safe access as long as it is oriented toward the targeted axis, even if there is a small deviation. Furthermore, the access along the axis of the calyx allows the working sheath straight forward into the pelvis, which potentially improves the mobility and vision field of the working sheath to reach a higher efficiency of stone clearance. In this study, the relative lower complications and higher stone-free rates may result from the appropriate direction of the renal access, which not only potentially reduces the risk of vascular injury but also improves the efficiency of lithotripsy.
In the present study, we found no statistically significant difference in hemoglobin reduction for mini-PCNL with Fr16, Fr18, Fr20, and Fr22 accesses, which is inconsistent with other studies. Previous research studies have shown that the bigger access size correlated with significant drop of hemoglobin, when the size changed from Fr22 to Fr30 [6, 7, 14]. Unsal et al. [15] also pointed out that the access size dilated to Fr24 or more may result in greater drop in the hemoglobin level in old children. There were a few possible causes. First, the larger access theoretically causes more parenchymal and, inadvertently, vascular injury especially when the size of the access is larger than Fr22. Second, when the access size exceeds Fr22, its mobility decreases significantly with the increase of the size, and it is more likely to tear the renal parenchyma and calyx by moving the working sheath during lithotripsy. Therefore, we hypothesized that the renal parenchyma could tolerate a limit of dilation and not be torn easily when the range of size is between Fr16 and Fr22, but beyond this limit, the renal parenchyma would be more vulnerable to injury due to excessive tension.
In our present study, there was significant decrease in the operative time according to the increase of access sizes from group Fr16 to Fr20. The reason may be that we used holmium laser lithotripsy and perfusion irrigation to remove the stone fragments. As we know, the bigger access was more efficient to remove stone for its size allows the relatively bigger fragments to rinse out, while the smaller access needs significantly longer time to fragmentize stone into the smaller pieces. However, there was no statistically significant difference in the operative time between group Fr20 and group Fr22. In our experience, the Fr22 access allows the larger stone fragments to escape than the Fr20 access, but it also requires a greater flow of fluid perfusion to maintain the pressure of reflux to remove fragments, which is usually difficult to achieve in the case of hydronephrosis, thus increasing the time consumed.
The total stone-free rate in this series was 93.6% (92.1–95.0%), which was as good as some contemporary studies have reported [12, 16, 17]. Stone-free rate is related to many factors; the location of puncture point and the choice of target calyx are the factors that can be controlled subjectively during PCNL [18-20]. According to the structure of collection system and stone distribution, selecting the right target calyx to build renal access can maximize the removal of stones. But, for the specific procedure of puncture, as mentioned above, the axis of the target calyx is an effective direction to improve the stone clearance rate and reduce the complications. The complications were rare in this series. The transfusion rate and postoperative fever were comparable among groups and similar to most of the previous reports [6, 7, 21]. Only 2 cases belonging to Fr18 and Fr20 groups observed delayed bleeding needing angioembolism. Delayed bleeding is considered to be the most common type of bleeding after PCNL and is usually associated with the formation of pseudoaneurysms in the renal access [22]. Both of the cases occurred during the removal of the nephrostomy tube, and the renal angiography revealed injury to an abnormal artery in the percutaneous access. Abnormal arteries are considered to occur within the renal pyramidal region and are usually seen in fused renal pyramids [5]. These abnormal arteries may be damaged during the establishment of percutaneous renal access and form pseudoaneurysms.
There are several limitations to the present study. First, this was a single-institution experience with a limited number of patients. A large multicenter randomized trial will be more informative. Second, the study only considered relatively simple kidney stones. For complex stones, such as staghorn stones, high-burden stones, and multiple stones, we usually choose Fr24 access plus EMS lithotripsy system or combined application of multiple accesses to improve surgical efficiency and stone clearance rate. Despite the abovementioned limitations, our study can highlight that access size-related bleeding was comparable during mini-PCNL with single access performed.
Conclusion
The collected data from the mini-PCNLs show the axis of target calyx was a reliable ultrasonic-guided marker for establishment of percutaneous renal access, and the different sizes of accesses did not affect the hemoglobin reduction, stone-free rate, complications, nephrostomy drainage, and hospital stay time. The operative time was significantly decreased with the increased size of access from Fr16 to Fr20; however, there was no significant difference between Fr22 and Fr20. Therefore, when we performed mini-PCNL, Fr16 to Fr22 accesses were available without considering the size-related bleeding; however, Fr20 access may be sufficient in terms of size-related efficiency.
Statement of Ethics
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All subjects have given their written informed consent, and the study protocol was approved by the institute’s committee on human research. The trial was approved by the local ethics and research scientific committee.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
The work was supported by grants from the National Natural Science Foundation of China (81870471 and 81800617) and the Science and Technology Major Project of Hubei Province (2019AEA170).
Author Contributions
Weimin Yu and Fan Cheng contributed to the conception of the study and performed the operations; Yuan Ruan and Zhuang Xiong contributed significantly to analysis and manuscript preparation; Yunlong Zhang and Ting Rao performed the data analyses and wrote the manuscript.
References
Additional information
Weimin Yu and Yuan Ruan contributed equally.

