

Abstract
Introduction: Studies comparing different single-use flexible ureteroscope (su-fURS) models are lacking. The objective was to compare three types of su-fURS: the Uscope 3022 (PUSEN), LithoVue (Boston Scientific), and EU-scope (Innovex). Methods: This was a retrospective study comparing the clinical outcomes from patients undergoing flexible ureteroscopy with one of the three su-fURS for upper urinary tract stone treatment between September 2019 and 2021. Analysis included total surgery and fluoroscopy time, post-procedure ureteral catheter, stone-free rate (SFR), and complications. Results: There were 104 cases with the Uscope 3022, 141 with LithoVue, and 80 with EU-scope. Groups were comparable in terms of stone size, location and density, and prior double-J stent presence. Multivariate analysis showed no difference in terms of SFR: 79% (Uscope 3022), 77.5% (LithoVue), and 81% (EU-scope); p = 0.38. Significant differences were found for total surgery and fluoroscopy time, as well as ureteral access sheath use (p < 0.001), favoring the EU-scope group. Discussion/Conclusion: The three devices evaluated are highly effective in treatment of kidney stones. Reasons for difference in total surgery and fluoroscopy time and access sheath use are not clear. However, this could be explained by technical aspects of these devices, such as external diameter, optical resolution, and field of view.
Introduction
Although use of a flexible ureteroscope was first reported by Marshall in 1964 [1], the concept of modern flexible ureteroscope was introduced by Bagley and Rittenberg in 1987 [2]. Remarkable technical improvements in flexible ureteroscopes have been made since 1990, and the first single-use flexible ureteroscope (su-fURS) was introduced in 2011 [3]. Several improvements in the image quality, external diameter, and deflection capacity of su-fURSs have been made by their manufacturers. Owing to the remarkable worldwide expansion of this technology, a large number of people have access to less invasive therapies. In addition, there exists sufficient evidence showing that su-fURS use yields results similar to those obtained with reusable fURS use [4‒7]. However, data regarding the clinical comparisons between different su-fURS models are lacking, and the majority of the related studies have focused on in vitro and ex vivo comparative evaluations. In 2018, our study group reported the first clinical evaluation of Uscope 3022 (PUSEN) [8]. The clinical results obtained using the Uscope 3022 were similar to those obtained using conventional reusable fURSs. Since then, several new su-fURS models have emerged on the market. In the present study, we present a comparison of the clinical performances of the Uscope 3022, LithoVue (Boston Scientific), and EU-scope (Innovex AnQing) su-fURSs.
Materials and Methods
Between September 2019 and 2021, this retrospective study was performed at Clinica Santa María, Santiago de Chile, which is a tertiary referral center for the treatment of complex urinary stones. All patients were evaluated by a urologist at the Comprehensive Center for Stone Disease at the hospital. Patients who underwent flexible ureteroscopy for upper urinary tract stones, were older than 18 years, and were able to provide consent for the procedure were included in this study. The exclusion criteria were known ureteral stricture, pregnancy, renal insufficiency, and active kidney infection. Upon recruitment, each patient provided written informed consent. All procedures involving human participants were performed in accordance with the ethical standards of the institutional and local scientific research ethics committees and with the 1964 Helsinki Declaration. All patients provided written informed consent. The procedures were performed by a urologist specializing in stone treatment. The patients underwent retrograde intrarenal surgery (RIRS) using one of the three su-fURSs: group 1 used Uscope 3022, group 2 used LithoVue, and group 3 used EU-scope. Considering the study design, the surgeon could not be blinded with respect to the su-fURS used; therefore, su-fURS selection was based on each su-fURS brand’s availability and individual operator preference on the day of surgery. The following information for each patient was collected from our regular database registry: demographic parameters, stone characteristics, surgical time (total time from the insertion of the endoscope, including cystoscopy, to the end of the procedure), total laser treatment time, fluoroscopy time (total time of irradiation, including double-J catheter placement, if necessary), stone-free rate (SFR), ureteral catheter use, and complications (according to the Clavien-Dindo classification). Moreover, data regarding scope failure (including loss of image quality), active deflection malfunction, and working channel problems were recorded. To reduce the bias related to surgeon familiarity with the use of each type of scope, the first 10 patients who underwent the procedure in each group were excluded from the analysis.
Preoperative evaluations included noncontrast computed tomography, urinalysis, and renal function tests. The patients underwent surgery under regional or general anesthesia, depending on each patient’s condition, in the lithotomy position. As part of our routine practice, a nitinol safety guidewire (0.038 in) was used in all the patients. A semirigid ureteroscope was then inserted using a second guidewire to achieve optic dilation of the distal part of the ureter. If adequate dilatation was not achieved with this maneuver, a double-J catheter was placed, and the definitive procedure was postponed for at least 10 days. A 12/14-Fr (Proxis, Bard) or 11/13-Fr (Navigator HD; Boston Scientific) ureteral access sheath was used when needed, depending on the local availability of the sheaths at the time of surgery. The selected su-fURS was advanced under endoscopic and fluoroscopic guidance. The kidney collecting system was visualized and evaluated before stone dusting was performed using a 273-μm holmium laser fiber (100-W high-power holmium laser; Lumenis). Depending on stone localization, a frontal open grasper (NgageTM; Cook Medical) was used to relocate the stones to a more favorable location for laser lithotripsy. At the end of the procedure, a double-J stent was placed if clinically significant residual stone fragments remained. The patients were evaluated as outpatients at 15 days, 30 days, and 3 months after the procedure. Stone-free status was defined as no evidence of stones or the evidence of fragments <2 mm on noncontrast computed tomography at 3 months. Statistical analysis was performed using Stata version 12.0 software. Continuous variables were analyzed using one-way analysis of variance or the Kruskal-Wallis test, and categorical variables were analyzed using Fisher’s exact test or χ2 test. Statistical significance was set at p < 0.05.
Results
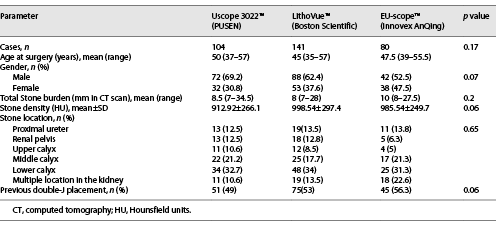
The inclusion criteria were met by 325 patients; of these patients, 104 were treated using the Uscope 3022, 141 were treated using the LithoVue, and 80 were treated using the EU-scope (Fig. 1). Patient and stone characteristics are presented in Table 1. The mean stone sizes for the Uscope 3022, LithoVue, and EU-scope groups were 8.5, 8, and 10 mm, respectively (p = 0.2). The mean stone densities, measured in Hounsfield units, in groups 1, 2, and 3 were 912.9, 998.5, and 985.5 Hounsfield units, respectively. General anesthesia was used in almost every case: 103 (99%), 139 (99%), and 80 (100%) of patients in groups 1, 2 and 3, respectively. No statistically significant differences in age, sex, stone location, and previous double-J stent placement were observed between the groups. The number of patients treated for lower pole stones did not significantly differ between the groups.

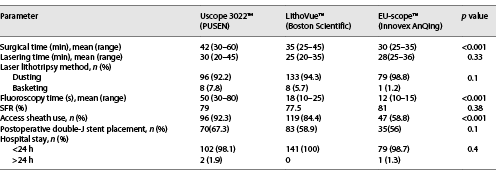
As described in Table 2, the total surgical time was significantly longer in group 1 (p < 0.001), but the total laser treatment time did not differ between the groups (p = 0.3). The total fluoroscopy time was shorter by 6 and 38 s in group 3 than in groups 2 and 1, respectively (p < 0.001). SFRs at the end of the follow-up period were slightly higher in group 3 (81%) than in group 1 (79%) and group 2 (77.5%), although the differences were not statistically significant (p = 0.4). Ureteral access sheaths were used in a higher number of patients in groups 1 and 2 (92.3% and 84.4% of the patients, respectively) than in group 3 (58.8% of the patients) (p < 0.001). The postoperative double-J stent placement rates were similar between the groups (p = 0.1). The most commonly used intracorporeal laser lithotripsy technique was dusting, which was used in >90% of the patients in all the groups (p = 0.1). Most of the procedures performed in the three groups required a 1-day hospital stay. Five patients developed postoperative complications. In group 1, a patient had prolonged hematuria, which was managed conservatively. In group 2, a patient required double-J stent replacement for pain management and another patient required intravenous antibiotic therapy for urinary tract infection on postoperative day 5. Further, in group 3, 2 patients had prolonged hematuria, which was satisfactorily managed conservatively.
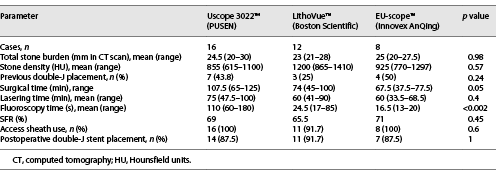
A subgroup analysis was performed to compare the results of the treatment of stones 20–30 mm in diameter between the groups. Patient demographic and stone characteristics were similar between the groups. Time measurements (surgical, lasering, and fluoroscopy times) showed results similar to those obtained in the whole-group analysis. As expected, SFRs were lower in the subgroup analysis than in the whole-group analysis but were similar between the groups; ureteral access sheaths were almost always used in all groups in the subgroup analysis (p = 0.6) (Table 3).
Discussion
One of the biggest advances in the field of endourology in the last 10 years has been the introduction of su-fURSs. Before that, several advances were made in ureteroscope design, including the introduction of ureteroscopes with smaller diameters, greater deflection in both directions, and the subsequent incorporation of digital technology. However, high purchase and maintenance costs and poor durability remain significant issues [5, 9, 10].
In this study, the clinical performances of three su-fURSs were compared. After a cost analysis at the beginning of 2017, the Urology Department of our hospital decided to mainly use disposable endoscopic equipment for upper urinary tract stone treatment and use reusable equipment in selected cases such as upper tract urothelial carcinoma diagnosis and treatment. The Uscope 3022 was the first su-fURS to be used by our department in June 2017. By the end of 2017, we started using the LithoVue, and by August 2019, we started using the EU-scope. Thereafter, all three su-fURS models were available for use. It is important to note that EU-scope is distributed as Axis (Dornier) in the US market. The three su-fURSs have similar technological characteristics. Their imaging systems, lengths, weights, working channel diameters, and deflection capacities are similar. However, the EU-scope provides digital images of a higher resolution owing to the CMOS image sensor [11, 12]. Moreover, the EU-scope has a slightly smaller outer diameter than the LithoVue and Uscope 3022. In our study, the preoperative patient demographic and stone characteristics were similar between the groups. However, some differences were evident in the intraoperative parameters. The surgical and fluoroscopy times were significantly longer in the Uscope 3022 and LithoVue groups than in the EU-scope group, but the lasering times did not differ significantly. A reason for this could be that a lower use of ureteral access sheaths led to a reduced need for fluoroscopy and consequently reduced the total surgical time in the EU-scope group. The reason for the lower use of ureteral access sheaths in the EU-scope group is unclear, considering that the main factors influencing access sheath use did not differ between the groups (mean stone diameter, lower pole stone incidence, and pre-stenting rate). However, the smaller diameter of the EU-scope could be associated with the lower use of access sheaths in the EU-scope group. Because cost considerations can often be a source of surgical bias, the easier passage of the thinner ureteroscope may have influenced the final decision of avoiding access sheath use.
However, in the subgroup analysis of patients with stones 20–30 mm in diameter, although access sheath use did not differ between the groups, the surgical and fluoroscopy times were shorter in the EU-scope group than in the Uscope 3022 and LithoVue groups. Another reason for these differences in time measurements could be poor image quality, which is a known limitation of su-fURSs; however, recent studies have reported otherwise. Marchini et al. [13]. reported that LithoVue outperformed Flex-X2 with respect to the resolution power and field of view, whereas Uscope 3022 outperformed Flex-X2 with respect to only resolution power. The main limitation of this study was its in vitro setting. Owing to an improvement in the CMOS image sensor of the EU-scope, it provides, in our opinion, the best image quality of all the su-fURSs available so far, and this could perhaps be the underlying reason for the shorter surgical and fluoroscopy times in the EU-scope group. Unfortunately, head-to-head trials focusing on this topic are lacking.
Another point of interest is the performance of su-fURSs in challenging cases, such as the treatment of patients with lower pole stones or stones measuring >2 cm in the largest dimension. Similar SFRs have been reported in patients with lower pole stones treated using su-fURSs and in those treated using reusable fURSs [14‒16]. The present study did not examine this topic in detail; however, similar numbers of patients with lower pole stones were treated in the three groups. Percutaneous nephrolithotomy is the recommended treatment option for patients with renal calculi >2 cm. Owing to recent technological advances in fURSs, several studies on RIRS for the management of large renal stones have reported promising results [17‒19]. In the present study, the SFRs in the three groups were slightly higher than those traditionally reported in patients treated using reusable fURSs [17, 20].
Although a retrospective study design is usually considered a limitation, we believe that the retrospective design of this study was an advantage for the real-world analysis. This is because a purely experimental design does not provide a precise evaluation of real-world daily practice. The main limitation of this study was the lack of an economic evaluation. This is largely explained by the great variability in the prices of medical supplies in this region of the world.
Finally, regarding su-fURS performance, the first European experience with LithoVue showed a 5% (2 patients) rate of malfunction [6]. However, no damage to the instrument (including deflection or image quality loss and working channel malfunction) was evident in the 325 patients included in the present study.
Conclusion
This retrospective study showed that RIRS using any one of the three evaluated su-fURSs in patients with upper urinary tract stones was safe, and intraoperative and postoperative parameters were similar between the three groups. Therefore, considering the clinical results, it is not possible to recommend one su-fURS brand over the other. Considering that countless new models and commercial brands of su-fURSs are likely to be introduced in the future, urologists must try to minimize biases and maintain a patient-centered approach.
Statement of Ethics
All procedures involving human participants were performed in accordance with the ethical standards of the Institutional and local Scientific Research ethics committees and with the 1964 Helsinki Declaration. Upon recruitment, each patient provided written informed consent. This study protocol was reviewed and approved by local “Scientific ethics committee,” belonging to Clínica Santa María, approval act number [19] (the name of the ethics committee is: “Comité Ético Científico de Clínica Santa María).”
Conflict of Interest Statement
Both the authors and contributors to this study have no conflict of interest to declare.
Funding Sources
No funding was received by any sponsor or source for the preparation of data for the manuscript for this study.
Author Contributions
Dr. José A. Salvadó: conceptualization, investigation, and wrote the manuscript. Dr. Vicente Elorrieta: wrote the manuscript, investigation, and analyzed the data. Dr. José M. Cabello, Dr. Renato Cabello: investigation and analyzed the data. Dr. Alfredo Velasco: wrote the manuscript and investigation.
Data Availability Statement
The data that support the findings of this study are not publicly available because they contain information that could compromise the privacy of research participants but are available from corresponding author JS on reasonable request.
