

Abstract
Introduction: The impact of teratomatous elements in orchiectomy specimens of metastasized testicular germ cell tumors (TGCT) regarding oncological outcome is still unclear. Methods: We performed a retrospective analysis including 146 patients with metastasized TGCT analysing patient characteristics. Results: Twenty-six (18%) of all patients showed teratomatous elements in the orchiectomy specimens. TGCT with teratomatous elements showed a significantly higher frequency of clinical-stage 2C-3 disease (73 vs. 49%, p = 0.031), visceral metastases (58 vs. 32%, p = 0.015), and poor prognosis (p = 0.011) than TGCT without teratomatous elements. Teratoma-containing TGCT revealed a significantly higher rate of post-chemotherapy retroperitoneal lymph node dissection (PC-RPLND, 54 vs. 32%, p = 0.041), with teratomatous elements being more often present in the PC-RPLND specimens (43 vs. 11%, p = 0.020) than nonteratoma-containing primaries. In the Kaplan-Meier estimates, the presence of teratomatous elements in orchiectomy specimens was associated with a significantly reduced relapse-free survival (RFS) (p = 0.049) during a median follow-up of 36 months (10–115.5). Conclusions: The presence of teratomatous elements in orchiectomy specimens is associated with an advanced tumor stage, worse treatment response as well as a reduced RFS in metastasized TGCT. Consequently, the presence of teratomatous elements might act as a reliable stratification tool for treatment decision in TGCT patients.
Introduction
Testicular germ cell tumors (TGCT) represent the most common solid malignancy in young men between the ages of 20 and 40 years [1]. Histologically they can be differentiated between seminomatous and nonseminomatous TGCT, of which nonseminomas may have 1 or more histological components, for example, teratomatous elements [1, 2]. Metastasized TGCT are classified according to the International Germ Cell Cancer Collaborative Group (IGCCCG) risk classification that reported 5-year survival rates depending on the anatomical localization of the primary (gonadal vs. extragonadal) and metastases (lymph nodes, pulmonary, and nonpulmonary metastasis) as well as tumor biology (tumor markers) [3-7]. The vast majority of metastasized TGCT is sensitive to cisplatin-based chemotherapy, resulting in cure rates of over 80% across all risk groups. However, cure rates depend on the IGCCCG risk classification, as approximately 10% of patients with a good prognosis, 20–30% with an intermediate prognosis, and 50–60% with a poor prognosis will nevertheless die from the TGCT [4, 6]. Furthermore, chemosensitivity seems to depend on the different histologic subtypes [8, 9]. As such, prior single-center studies revealed that nonseminomatous TGCT with teratomatous elements in the orchiectomy specimens are associated with a worse response to systemic therapy and have an increased probability of a post-chemotherapy retroperitoneal lymphadenectomy (PC-RPLND) compared to TGCT without teratomatous elements in the orchiectomy specimens [10-12]. Furthermore, TGCT with teratomatous elements had a higher risk of metastases than nonteratoma-containing primaries [12, 13]. However, the influence of teratomatous elements in the primary tumor on relapse-free survival (RFS), especially regarding up-to-date treatment options, remains unclear. Consequently, the aim of this study was to analyze the impact of teratomatous elements in orchiectomy specimens of metastasized TGCT regarding clinical stage, treatment options as well as follow-up.
Materials and Methods
Study Population
We retrospectively analyzed the TGCT database at the University Hospital of Cologne as an observational cohort study. 146 patients diagnosed with metastasized TGCT (ICD-10 code C62) that were referred to our department between 2014 and 2019 due to their initial diagnosis of TGCT or for follow-up visits of an existing TGCT are included in the study. We collected data on age, histology, clinical stage, and IGCCCG risk classification. Moreover, the type and duration of treatment as well as follow-up analyses were analyzed. Survival time was available for 130 patients. Subgroup analysis regarding the presence of teratomatous elements in the orchiectomy specimens was performed. Nonseminoma patients with seminoma elements in the primary as well as patients with pure seminoma were included in the study. Our study complies with the Declaration of Helsinki and local Ethics Committee approval was obtained (20-1229).
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY, USA). Continuous variables are presented as median (25th–75th percentile), categorical variables are given as n (%). Mann-Whitney U test for a pairwise comparisons of continuous variables and Pearson’s χ2 test for categorical variables. RFS and overall survival (OS) were estimated using the Kaplan-Maier method and compared patients with and without teratomatous elements in the orchiectomy specimens using the log-rank test. All reported p values are 2-sided, and p values <0.05 were considered statistically significant.
Results
Description of Study Population
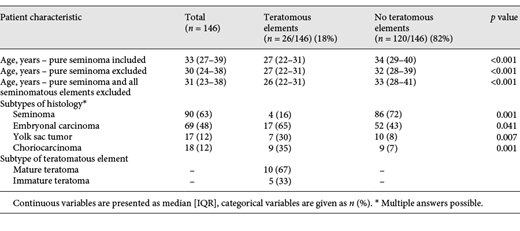
Of the eligible 146 patients with metastasized TGCT, 26 (18%) showed teratomatous elements in the orchiectomy specimens (Table 1). We first evaluated the age of our cohort of patients analysing (A) the whole cohort of patients (n = 146), (B) the whole cohort of patients excluding pure seminoma in the orchiectomy specimens (n = 83), and (C) the whole cohort of patients excluding pure seminoma as well as nonseminoma patients with seminoma elements in the orchiectomy specimens (n = 56). In all groups, patients with teratomatous elements were significantly younger compared to those patients without teratomatous elements (p < 0,001, Table 1). The whole cohort of patients (A) showed a median age of 33 years (27–39), while both subgroups of patients were younger (B: 30 years [24–38]; C: 31 years [23–38]).
Histological Characteristics
First, we compared the histological characteristics of patients with teratomatous elements to those without teratomatous elements in the orchiectomy specimens (Table 1). Regarding the occurrence of nonteratomatous elements in the orchiectomy specimens, seminomatous elements were predominantly found (63%), followed by embryonal carcinoma (48%), yolk sac tumor (12%), and choriocarcinoma (12%; Table 1). Teratoma-containing orchiectomy specimens showed a significantly higher co-occurrence of embryonal carcinoma (65 vs. 43%, p = 0.041; Table 1), yolk sac tumor (30 vs. 8%, p = 0.007; Table 1), and choriocarcinoma (35 vs. 7%, p < 0.001; Table 1) than tumors without teratomatous elements, but a significantly lower co-occurrence of seminoma (16 vs. 72%, p < 0.001; Table 1). According to a prior existing classification, mature teratoma was found in 67% of all orchiectomy specimens with teratomatous elements compared to immature teratoma, which was identified in 33% (Table 1).
Clinical Stage and IGCCCG Risk Classification
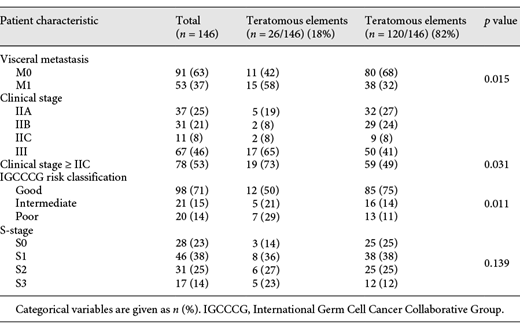
We next evaluated the clinical stage as well as prognostic group according to the IGCCCG risk classification system (Table 2). Here, TGCT with teratomatous elements showed a significantly higher frequency of clinical-stage 2C-3 disease (73 vs. 49%, p = 0.031; Table 2) as well as visceral metastatic disease (58 vs. 32%, p = 0.015; Table 2) than TGCT without teratomatous elements. Furthermore, teratoma-containing TGCT was associated with a significantly higher frequency of IGCCCG poor prognosis than nonteratoma-containing primaries (p = 0.011; Table 2). However, we did not find any significant differences regarding the s-stage (Table 2).
Treatment Options
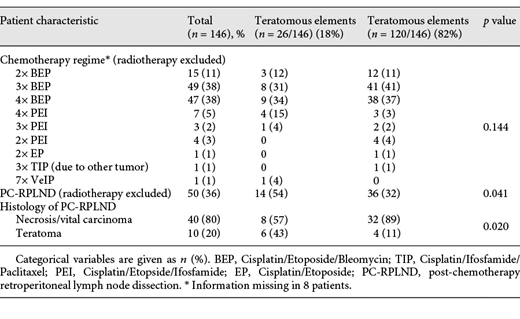
Regarding treatment options, patients with teratomatous elements revealed a significantly higher rate of retroperitoneal lymph node dissection after chemotherapy (54 vs. 32%, p = 0.041; Table 3) than TGCT without teratomatous elements. Here, patients with teratomatous elements in the orchiectomy specimens showed significantly more often teratoma in the PC-RPLND specimens (43 vs. 11%) than TGCT without teratomatous elements in the orchiectomy specimens (p = 0.020, Table 3). There was no difference in the chemotherapy regime used in the study population (p = 0.144, Table 3). Residuals after PC-RPLND occurred in 1/50 patient (2%), leading to disease progression during follow-up. 9 patients (9/146) were primarily treated with radiotherapy.
RFS and Overall Survival
The analysis of study population revealed that 9/22 (41%) patients with teratomatous elements in orchiectomy specimens relapsed compared to 18/108 (17%) patients without teratomatous elements (p = 0.032). In the Kaplan-Meier estimates, the presence of teratomatous elements in orchiectomy specimens was associated with a significantly reduced RFS (p = 0.049, Fig. 1). The median time of follow-up with respect to RFS was 36 months (IQR: 10–115.5). The median RFS for teratoma-containing TGCT was 240 months compared to 114 months for nonteratoma-containing primaries. Thus, patients with teratomatous elements showed a trend toward higher rates of late relapses after 2 years than patients without teratomatous elements in the orchiectomy (p = 0.053). One (5%) of all patients with teratomatous elements and 8 (6%) of all patients without teratomatous elements deceased during follow-up. Until the end of follow-up, the presence of teratomatous elements had no impact on the OS (p = 0.534), however, the median OS was not reached. Similar results were found in the subgroup analysis that excludes pure seminoma (RFS: p = 0.021, see online suppl. Fig. 1; for all online suppl. material, see www.karger.com/doi/10.1159/000515715; OS p = 0.788).

Kaplan-Meier estimates for RFS of study population comparing patients with and without teratomatous elements in orchiectomy specimens (n = 130). IGCCCG, International Germ Cell Cancer Collaborative Group; IQR, Interquartile range; PC-RPLND, post-chemotherapy retroperitoneal lymphadenectomy; RFS, relapse-free survival; TGCT, testicular germ cell tumors.
Kaplan-Meier estimates for RFS of study population comparing patients with and without teratomatous elements in orchiectomy specimens (n = 130). IGCCCG, International Germ Cell Cancer Collaborative Group; IQR, Interquartile range; PC-RPLND, post-chemotherapy retroperitoneal lymphadenectomy; RFS, relapse-free survival; TGCT, testicular germ cell tumors.
Discussion/Conclusion
Besides clinical stage and IGCCCG risk classification, treatment response seems to depend on the different histologic subtypes, especially the presence of teratoma [10-13]. In our study, we showed that TGCT with teratomatous elements in the orchiectomy specimens is more likely to have an advanced tumor stage than TGCT without teratomatous elements. Furthermore, teratoma-containing primaries showed a lower remission rate after chemotherapy, leading to a higher rate of teratoma in the PC-RPLND specimens as well as a significantly reduced RFS compared to nonteratoma-containing primaries. Currently, there are only very few clinical studies available analyzing the possible influence of teratomatous elements of nonseminomatous metastasized TGCT regarding the treatment response as well as follow-up analysis [10-15].
First, we evaluated the presence of nonteratomatous elements in teratoma-containing orchiectomy specimens. Here, we revealed a higher co-occurrence of choriocarcinoma, embryonal carcinoma as well as yolk sac tumor, but a lower co-occurrence of seminoma together with teratomatous elements. In contrast to these results, a prior study including 118 nonseminomatous TGCT patients described that the occurrence of teratomatous elements was most frequently associated with choriocarcinomatous elements [13]. As this is the only study available in literature, a connection between the co-occurrence of the histological subtypes is difficult to draw. Another prior study of our working group revealed that all patients with metastasized teratoma showed microfocal nonseminomatous components or a burned-out tumor in the orchiectomy specimens after a detailed review of the primary tumor of initially supposed pure testicular teratoma [14]. Describing the malignant potential of pure mature teratoma, we thus recommend a detailed pathohistological analysis of serial sections of all orchiectomy specimens.
PC-RPLND is performed as part of the guideline-recommended multimodal therapy of advanced TGCT with residual masses >1 cm [1, 2]. Histopathological analysis revealed that 30–60% and 8–25% of the residual tumors harbor teratoma or vital carcinoma in the PC-RPLND specimens [1, 2]. Regarding the subgroup analysis of orchiectomy specimens, TGCT with teratomatous elements showed a lower remission rate after chemotherapy and thus a higher rate of teratoma in the PC-RPLND specimens than TGCT without teratomatous elements [10-15]. In line, a retrospective review performed by the Indiana University including 644 patients, found teratoma elements in the PC-RPLND specimens in 86% of all teratoma-containing primaries compared to only 48% of all nonteratoma-containing primaries [11]. Furthermore, a prior study of our working group described the malignant potential of patients with supposedly pure testicular teratoma in the orchiectomy specimens and found a significant histology (3 teratomas, 1 choriocarcinoma, and 1 malignant somatic transformation) in the PC-RPLND specimens in 83% of all cases [14]. Another study analyzing specimens of primary RPLND described positive lymph nodes in 43% of all primary RPLND specimens, of which 30% contained teratomatous elements [12]. Furthermore, our study revealed that teratoma-containing primaries were associated with an advanced tumor stage namely a significantly higher frequency of clinical-stage 2C-3 disease, visceral metastatic disease, and higher frequency of poor prognosis. A prior study on 118 TGCT patients came to a similar conclusions, as they showed teratoma-containing primaries to have an almost 5-fold higher risk of metastases than nonteratoma-containing primaries [13]. Taken together, these analyses clearly demonstrate that teratoma-containing primaries represent tumors with a high risk for metastatic disease as well as significant histology (teratoma or vital carcinoma) in the RPLND specimens. Consequently, PC-RPLND should be performed in teratomatous-containing primaries, especially in case of residual masses >1 cm [1]. However, the absence of teratomatous elements in the orchiectomy specimen do not reliably predict the absence of teratoma in the PC-RPLND specimen. Therefore, the EAU guidelines currently recommend a PC-RPLND in case of residual masses >1 cm after chemotherapy irrespective of the presence or absence of teratoma in the orchiectomy specimen [1].
In a retrospective single-center study on 193 patients with metastatic nonseminomatous TGCT and a median follow-up of 17 (0.3–35) years, patients with teratomatous elements in the orchiectomy specimens had a higher tumor-specific mortality rate than TGCT without teratomatous and seminomatous elements (27.4 vs. 17.4% vs. 10.3%, p = 0.03) [15]. Furthermore, the mortality rate of TCGT patients with teratomatous elements in the primary tumor was associated with chemoresistance, the presence of nonteratomatous tumor elements, and an increased frequency of extraperitoneal visceral metastasis [15]. In our study, a reduced OS has not been demonstrated. As this might be due to the relatively short follow-up, future analysis will lead to similar results. However, our study for the first time analyzed the influence of teratomatous elements in orchiectomy specimens on RFS and described it as significantly reduced during a median follow-up of 36 months. Furthermore, patients with teratomatous elements showed a trend towards higher rates of late relapses after 2 years than patients without teratomatous elements in the orchiectomy. Consequently, a guideline concordant treatment as well as follow-up is of utmost importance in order to optimize the RFS in this cohort of patients [1].
Although our study is one of the largest studies with a contemporary patient cohort, the limitation of this study is its retrospective design and the relatively short follow-up, thus missing to reach a median OS. Given that this is a single-center series, our findings need validation in an independent cohort. In order to further corroborate with the beforementioned findings, we initiated a national register study to be realized within the German Testicular Cancer Study Group which also includes a translational project of gene expression and immunohistochemical aspects.
Taken together, our study revealed that the presence of teratomatous elements in orchiectomy specimens is associated with an advanced tumor stage, worse treatment response as well as a reduced RFS in metastasized TGCT. Therefore, PC-RPLND remains the standard approach in patients with residual masses >1 cm of metastatic nonseminomatous TGCT. However, in the future, presence of teratomatous elements might act as a reliable stratification tool for PC-RPLND.
Statement of Ethics
Our study complies with the Declaration of Helsinki and local Ethics Committee approval was obtained (20-1229).
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Contributions
Paffenholz P.: Project development, data collection or management, data analysis, manuscript writing/editing. Nestler T.: data collection or management, and manuscript editing. Maatoug Y.: manuscript editing. Brandenstein M.: manuscript editing. Köditz B.: manuscript editing. Loosen S.H.: data analysis and manuscript editing. Fischer N.: manuscript editing. Pfister D.: manuscript editing and supervision. Heidenreich A.: project development, manuscript editing, and supervision.

