

Abstract
Background: Topical therapy of nonmuscle-invasive bladder cancer (NMIBC) is based on immunotherapy with Bacillus Calmette-Guerin and chemotherapy administered by passive instillation, but an active drug administration achieves a better concentration of the drugs in the bladder. Aim: This study aimed to investigate the effectiveness of electromotive drug administration (EMDA) of mitomycin C (EMDA/MMC) in intermediate- and high-risk NMIBC patients 6 months after the end of induction treatment. Materials and Methods: Sixty-five patients diagnosed with histologically confirmed NMIBC, with a complete transurethral resection of all visible tumors underwent EMDA/MMC. Primary endpoint was the proportion of responders at 3 or 6 months. Results: Data on follow-up were available for 62 subjects at 3 months and 45 at 6 months. EMDA was effective in intermediate- and high-risk patients: because of the small number of cases no conclusions can be drawn on the efficacy in the low-risk group. No difference in the response to treatment between intermediate- (83.3%) and high-risk (84%) patients could be seen. Conclusions: EMDA/MMC is a useful technique for an effective and safe treatment of primary and recurrent NMIBC, and a valuable therapeutic option in intermediate- and high-risk NMIBC patients.
Nonmuscle-invasive bladder cancer (NMIBC) is a heterogeneous disease, with frequent relapses and potentially progressive, invasive, undifferentiated forms sometimes affecting the muscle layers of the bladder [1].
In NMIBC patients, endoscopic resection of the neoplastic tissue, followed, if needed, by intravesical immunotherapy and/or chemotherapy, has so far been the first-line treatment since >40 years. The first-line pharmaceutical treatment of NMIBC in high-risk patients is still the Bacillus Calmette-Guerin (BCG) immunotherapy [2]. Until approximately 20 years ago, pharmacological treatment was based on the passive diffusion of the drugs used, mainly mitomycin C (MMC) and epirubicin, by infusing the drug dissolved in a saline solution into the bladder and allowing it to penetrate the bladder mucosa during approximately 2 h. More recently, pharmacological treatment has evolved toward the use of devices that allow the drug to actively enter the bladder mucosa [3‒10]. Presently, the 2 main methods used to achieve an active diffusion are thermochemotherapy, which is carried out using catheters that increase the temperature of the bladder up to 43°C [11], and the electromotive drug administration (EMDA), which induces an ionophoresis of the drug used [3]. EMDA is very easy to use and can be carried out in an outpatient setting during 20 min sessions.
Previous studies were carried out with sequential therapy (EMDA/MMC + BCG) and only in high-risk NMIBC patients [12]. We thus decided to carry out a multicenter, retrospective study aiming to assess whether a treatment with EMDA/MMC alone may achieve a complete response at 3 or 6 months in patients with nonmuscle-invasive urothelial carcinoma of the bladder.
Methods
Data Source and Study Population
Patients entered the study between April 2016 and July 2018 in one center in Switzerland (R.C.) and one in Italy (M.Z., G.M.L., S.C.). The local Ethics Committee approved the study (decision no. 2018-01470/CE 3390), and consent was obtained from all patients involved.
We evaluated NMIBC patients who were treatment naïve or were refractory to other treatments. They underwent a 30-min treatment with EMDA/MMC (Physion Mini 30N2, 20–23 mA, 40% [w/v] mitomycin in distilled water). Patient demographics, severity of carcinoma (at the time of first diagnosis and start of EMDA treatment), previous treatments, number of comorbidities, number of instillations, maintenance phase, and response to the treatment after 3 and 6 months were recorded.
Statistical Analysis
Primary endpoint was the proportion of responders at 3 or 6 months for the different severity of carcinoma (low, intermediate, and high risk) at the start of EMDA treatment. Response was defined as a negative cystoscopy, cytology, and/or histology at least one of the 2 time points. Cases with a negative cystoscopy and histology at 3 months but a positive outcome at 6 months were defined as nonresponders. The endpoint was investigated using the Fisher’s exact test.
We created dichotomous variables (no = 0, yes = 1) for the outcome responder/not responder at 3 and at 6 months and categories (low risk = 0, intermediate risk = 1, high risk = 2) for severity of carcinoma at enrollment and start of EMDA treatment. Risk categories were defined as set out in the current updated European Association of Urology guidelines for NMIBC [13, 14].
Demographic data and cystoscopy results at 3 and 6 months are presented only descriptively. Proportions are displayed with their 95% CI, nonparametric data using medians and interquartile ranges, and continuous data with means and 95% CI.
The association between binary and categorical variables was investigated using the Fisher’s exact test and between continuous variables with the nonparametric test of U Mann-Whitney because normality of the distributions could not be shown. All tests were two-tailed and considered significant at p < 0.05. All statistical analyses were performed using IBM SPSS 21.0 for Windows (IBM, Armonk, NY, USA).
Results
Patient Disposition and Demographics
The patients’ disposition is presented in Figure 1 and the demographic data in Table 1. Sixty-five patients were treated in the 2 centers between April 2016 and July 2018. Sixty-two (93.8%) of them were treated with at least 4 instillations under the EMDA protocol and were included in the analysis. As one center (R.C.) included only 10 patients versus 55 in the second one, no distinction between the 2 centers was made and only the aggregate results are presented.
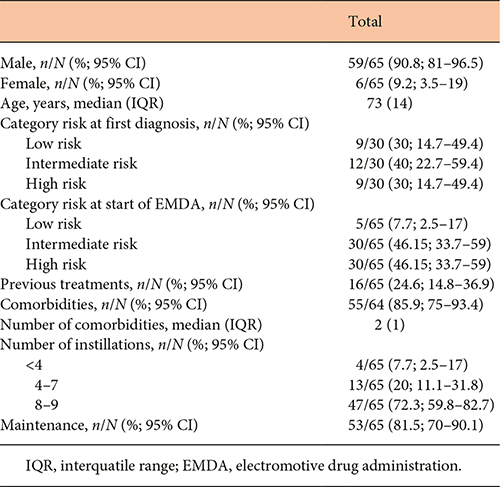

Of the 65 evaluable patients 59 were men and 6 women. The median age in years (interquartile range) was 77 (10) and 72 (15), respectively. Only 5 patients at low risk started the EMDA/MMC treatment, as compared to 30 at intermediate and 30 at high risk.
Sixteen patients had already undergone a passive treatment with MMC or BCG before receiving EMDA/MMC and 2 of them had already had a previous EMDA/MMC therapy. Four patients (6.2%) received <4, 14 (21.5%) 4–7, and 47 (72.3%) 8 instillations during the induction period with EMDA/MMC. Fifty-three patients (88.5%) continued with a maintenance therapy after successful induction.
Primary and Secondary Endpoints
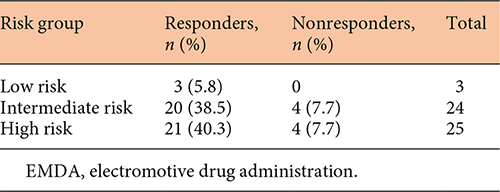
The results of the analysis of the proportion of responders (negative cystoscopy, citology and/or histology either at 3 or 6 months) and nonresponders are presented in Table 2. EMDA was effective in all 3 risk groups, with statistically significant differences in the rate of responders versus nonresponders (p = 0.000), but the number of evaluable low-risk subjects (n = 3) does not allow drawing any conclusions for this risk group. No statistically significant difference could be seen in the response rates between intermediate- (83.3%) and high-risk (84%) patients.
Proportion of responders and nonresponders after end of induction with EMDA. No difference in efficacy between the intermediate- and the high-risk group can be observed. Low-risk patients have not been included in the statistical analysis and are included only descriptively in the table
Data on the follow-up at 3 months were available for 62 subjects, of whom 54 were responders. The proportions of intermediate- and high-risk patients at start of the EMDA protocol were similar in both responder (44.5% intermediate, 48.1% high risk) and nonresponder groups (50% intermediate, 50% high risk), with no statistically significant difference (Table 3).
Comparison between characteristics of responders and nonresponders at 3 and 6 months follow-up
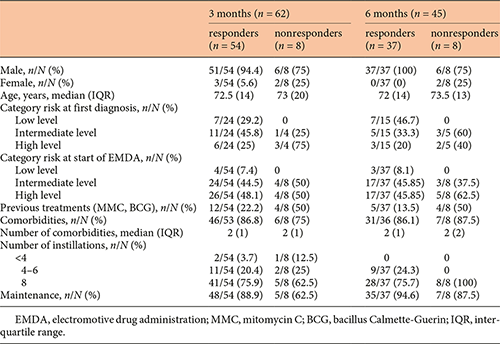
Data on the follow-up at 6 months were available for 45 subjects, of whom 37 were responders. Within the responders, the proportion of intermediate- and high-risk patients at start of EMDA treatment was the same (17/37; 45.85%). Thirty-seven responders at 6 months were already responders at 3 months, and 7 patients who were responders at 3 months had a relapse at 6 months. Only one patient was a nonresponder at 3 and 6 months.
Safety
In our study, we observed only 6 adverse events, that is, skin erythema in 3 patients, intolerance to catheter in 1, and bladder tightness and pain in 1 patient. Treatment had to be stopped only in the last instance, suggesting that EMDA is at least as safe as chemohyperthermia (CHT).
Discussion
This study confirms the efficacy of electro-mediated MMC in the topical treatment of NMIBC. Previously published studies documented similar results with EMDA/MMC in terms of efficacy in NMIBC patients, with almost identical success rates [6‒8, 12, 15, 16]. Overall, both EMDA and CHT appear to be effective. For instance, a study comparing CHT and BCG treatment reported a recurrence-free survival of 78.1% in the CHT group compared to 64.8% in the BCG group (intention-to-treat analysis) after 24 months [17].
With regard to CHT safety, for instance, adverse events observed by Arends et al. [17] included bladder spasms and pain in 14.4%, dysuria in 11.7%, nocturia in 10.3%, and urinary frequency in 9.9% of the patients after treatment in the CHT group. In the BCG group, the most prevalent adverse effects were urinary frequency (18%), dysuria (15%), nocturia (14.9%), and haematuria (11.2%).
CHT, however, is apparently associated with a slightly higher toxicity than EMDA [4]. Toxicity has been used as a primary endpoint by Geijsen et al. [18] in a clinical study carried out using invasive regional 70 MHz hyperthermia and MMC. In this study, 10% of the patients experienced a grade 2 toxicity (bladder complaints and lower back pain) and no grade 3 and 4 toxicities, but 6 of the 18 patients treated discontinued the therapy because of physical complaints, including MMC allergy. Inman et al. [19] did also not report any grade 3 or higher toxicities after CHT, and Longo et al. [20] concluded that the local toxicity induced by various thermochemotherapy techniques in high-risk NMIBC patients is acceptable, the benefit/risk ratio being positive when considering the response rates obtained.
In a comparative study, the local toxicity, assessed using a nonvalidated questionnaire, was higher in the CHT group than in the EMDA/MMC group [4]. In another, preliminary, small study carried out in 22 patients [21] EMDA, when used for various indications (NMIBC, local anesthesia for endoscopic bladder surgery, hydrodistension for the treatment of chronic noninfectious cystitis) was associated with the insurgence of 1 bladder ulcer (1% of all treatments), 14 bladder contractions (15.4%), and 4 moderate pain episodes (4.4%). Seven patients (31.8%) reported no side effects. This is in accordance with the results of our observations, as the adverse events observed in our study were mainly of mild intensity and only in one case a treatment needed to be stopped.
This study has some limitations. The number of patients that could be included and observed is still limited, and a longer follow-up time, presently ongoing, is needed to assess the long-term efficacy of the treatment. Further, there is a need to better define the ideal therapeutic regimen in terms of number of instillations and duration of induction and maintenance. Nevertheless, our results provide an indication that EMDA/MMC can be safely and effectively used in both intermediate- and high-risk patients. Low-risk patients are usually not in need of further therapies [13], and in our study, only 5 were considered by the physicians to potentially benefit from EMDA/MMC.
BCG has been increasingly used since 2004 and up to 2012, but since the major interruptions in BCG supply in 2011 and 2012 its therapeutic application appears to have decreased [22]. In fact, the doses used in NMIBC treatment are very high compared with those used for vaccination, and the current shortage for bladder cancer treatment may remain an issue in the future. In addition, the fermentation process employed to produce BCG has not changed since it was first described by Calmette and Guerin in 1921: genetic mutations introduced to BCG by repeated serial inoculation passages, as well as nonstandardization of BCG manufacture make its application in bladder cancer treatment unreliable [23].
Conclusions
EMDA/MMC is an interesting and effective alternative to other options for the intravesical therapy of NMIBC. It is easy to perform, and the results of several studies suggest that it may be more effective than the passive instillation of MMC, possibly also in BCG refractory diseases. It can be easily performed in an outpatient setting and it is well tolerated and fast, requiring approximately 20 min for each session.
Acknowledgments
We acknowledge the help by PD Dr. Orlando Petrini, Breganzona, Switzerland and Dr. Paola Gandolfi-Decristoforis, Cresciano, Switzerland in the statistical analysis and preparation of the final manuscript.
Statement of Ethics
The local Ethics Committee approved the study (decision no. 2018-01470/CE 3390), and consent was obtained from all patients involved.
Disclosure Statement
The authors have no conflicts of interest to declare.
Author Contributions
All authors contributed equally to data collection and preparation of the manuscript.
