

Abstract
Objectives: To assess the improvement of symptoms by sacral neuromodulation (SNM) in an objective way by carrying out an ambulatory urodynamic study (ambulatory-UDS). Until now, successful treatment has been defined as a ≥50% improvement recorded on voiding diaries. Voiding diaries are a patient reported outcome tool. A tool with less bias is desired to evaluate the treatment results before an expensive permanent system is implanted. Methods: Between 2002 and 2015, a total of 334 patients with lower urinary tract symptoms were included consecutively in an ambulatory-UDS database. From this database, a subgroup of patients was selected which underwent SNM. Results: In 51 patients, an ambulatory-UDS was performed both at baseline and during the SNM test period. A positive treatment outcome after test stimulation based on the patients’ voiding diary, correlated (p < 0.0001) with an improvement on ambulatory-UDS. Twenty-six of the 30 patients, who have showed improvement of more than 50% on voiding diary parameters and who had subjective improvement of their symptoms, showed an early improvement on ambulatory-UDS. Conclusions: Ambulatory-UDS can be used in clinical decision making, as it is associated with voiding diary improvement during the SNM test period. Using ambulatory-UDS to confirm success could in the future justify the shortening of the test period.
Introduction
In this study, we investigated the value of an ambulatory urodynamic study (ambulatory-UDS) for the evaluation of treatment effect during the test evaluation period in sacral neuromodulation (SNM). Since the 1990s SNM is a recommended treatment in patients with overactive bladder syndrome (OAB) or non-obstructive urinary retention (NOR), for cases where conservative treatments failed or adverse events prevented therapy continuation [1]. As this treatment is invasive and expensive, a standard testing period is applied before embarking on a permanent implantation. Often eligible patients are affected by NOR or OAB for several years or even decades [2]. In general, treatment success of SNM is assessed by voiding diaries, subjective patient improvement, quality of life scores and symptom score questionnaires [1]. The final clinical decision concerning treatment success is dependent upon voiding diaries in most treatment centres and this is in line with the recommendation by most experts in the field. SNM success is therein defined as a reduction of one or more voiding symptoms with ≥50%, compared to the baseline situation. Although voiding diaries have been proven to be a reliable tool, they remain patient reported and hence will introduce inevitable bias. It is preferable to assess improvement of symptoms in a standardised and more objective (unambiguous) way.
In the past, an association between an improvement on a cystometrogram and the SNM treatment outcome was suggested. A significant correlation was found between improvement in symptoms and changed conventional-UDS recording in patients with NOR [3-5]. Similar significant correlations in OAB patients treated with SNM have been reported [6-8]. Unfortunately to date no comprehensive and objective assessment method has been developed for treatment evaluation. One of the reasons for this might be the situational sensitivities of conventional urodynamics that prevents a detection of representative changes [9]. The use of ambulatory-UDS may be a helpful tool to objectively assess the improvement of symptoms and overcome the hurdles of a conventional-UDS.
An ambulatory-UDS is defined as a functional assessment of the lower urinary tract: monitoring storage and voiding, utilising natural filling while the subject’s every day activities are reproduced [10]. The first to establish ambulatory-UDS was Comarr [11]. Since its development and a more widely use of ambulatory-UDS in the 1990s [12], a reasonable number of studies have been performed to assess the applicability of ambulatory-UDS in clinical practice. Ambulatory-UDS was standardised in 2,000 [10], but is yet to be validated clinically.
In this paper, treatment-induced changes on ambulatory urodynamic studies in patients treated with SNM are reviewed. The aim of this study is to explore to what extent the improvement in ambulatory UDS recordings can be used in the clinical decision making.
Methods
Patient Selection
From December 2002 until April 2015, a total of 334 patients with lower urinary tract symptoms were included in a consecutive ambulatory-UDS database. From this database, a subgroup of patients was selected, who underwent ambulatory urodynamic monitoring prior to and during the test period for SNM. Urodynamic results were related to treatment evaluation. Clinical informed consent was obtained from all patients for the additional ambulatory-UDS. The approval of the Medical Ethical Committee of Maastricht University Centre was obtained.
Urodynamic Studies
All urodynamic measurements were performed with use of Medical Measurements Systems (MMS B.V., Enschede, the Netherlands) equipment and according to the standardisation report of the ICS [10, 13]. An initial ambulatory-UDS was conducted in all following cases: (1) low quality conventional-UDS (2) assumed OAB without detrusor overactivity (DO) on conventional-UDS (3) incontinence with unclear primary origin or (4) suspected bladder acontractility and (5) enuresis nocturna. When an ambulatory-UDS had been performed to clarify the diagnosis and this patient underwent subsequent SNM treatment, a second ambulatory-UDS was used to compare to baseline to possibly confirm either success or failure during the test period.
The quality of all ambulatory-UDS recordings was ascertained and the full results were interpreted by an urologist specialised in urodynamics and a urology resident experienced in evaluating urodynamic measurements. Both were blinded to the SNM outcome. Standard definitions were adhered to when judging the measurements.
Any phasic contraction during the filling phase with rise and fall in detrusor pressure is diagnostic of DO. The ICS definition does not specify a minimum change in detrusor pressure, although waves of amplitude less than 5 centimetre H2O are difficult to detect. Bladder acontractility was defined as a filling and voiding phase without detrusor pressure rise. Hypocontractility was identified as a low detrusor pressure (less than 10 cm H2O) during the voiding phase, relative to the degree of obstruction, not resulting in (efficient) micturition. In case of a conventional-UDS, the hypocontractility definition is elaborated with a peak flow rate (Qmax) of less than 10 mL/s, voided volume should be greater than 100 mL and residual urine volume greater than 150 mL [14]. For ambulatory-UDS standardised limits have not yet been established [15]. In Figure 1, an example of an ambulatory-UDS work place set up is shown.

Ambulatory urodynamic study set-up. a The luna wireless module for registration of events during the ambulatory-UDS. b Solar measurement system. c A patient equipped with measurement catheters and the Luna mobile device. d An example of one part of ambulatory-UDS recording.
Ambulatory urodynamic study set-up. a The luna wireless module for registration of events during the ambulatory-UDS. b Solar measurement system. c A patient equipped with measurement catheters and the Luna mobile device. d An example of one part of ambulatory-UDS recording.
Sacral Neuromodulation Treatment
SNM treatment success was defined as a reduction of one or more micturition symptoms to ≥50%, compared to baseline, determined by comparing voiding diaries. An SNM test period using the tined lead procedure covered 4 weeks. Every included patient served as their own control.
Statistical Analysis
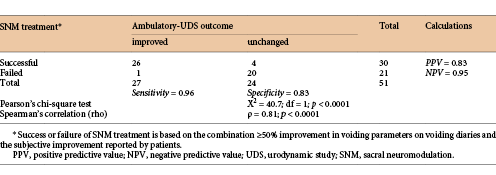
Descriptive and comparative statistics were calculated with the use of SPSS, IBM corporation, version 22. The median and 25–75 percentile interquartile range were described. Pearson’s chi-square test, Spearman’s correlation, the positive and negative predictive value, sensitivity and specificity were calculated.
Results
In 51 patients (32 women and 19 men), an ambulatory-UDS was performed at baseline and during the SNM test period. The mean age was 48.7 (SD 12.1): men were 52.1 (SD 12.3) and women were 46.6 (SD 11.7). Age was not statistically different between men and women (t test, p = 0.893). Most patients presented at the outpatient clinic with voiding LUTS, 37 of those had NOR, of which 17 were experiencing complete urinary retention and 20 were able to void more or less spontaneously but were still in need of catheterisation multiple times a day. An additional 10 patients had OAB complaints, 9 out of 10 were affected by OAB with urgency incontinence; one patient was continent. The remaining 4 patients presented with a combination of voiding and storage LUTS. In these patients, no neurogenic conditions could be objectified. Out of the total group of 51 patients, 30 (59%) showed an improvement of ≥50% on voiding diary parameters and reported subjective improvement of symptoms. These 30 patients received a definitive SNM implant. In the remaining 21 patients, the stimulating electrode was removed at the end of the test period, as no symptom improvement occurred (see Table 1). A neuromodulator was implanted in 80% (8/10) of the OAB group, 54% (20/37) of the NOR group and 50% (2/4) of the patients with combined symptoms.
Ambulatory measurements from the baseline and testing period recordings in the unsuccessful patients
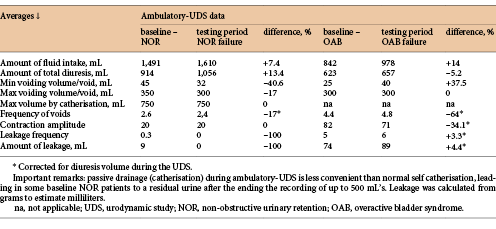
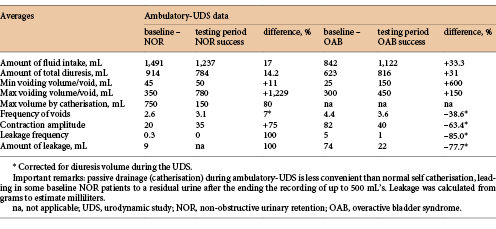
A positive treatment outcome after test stimulation based on voiding diaries, correlated (p < 0.0001) well with an improvement on ambulatory-UDS (Table 2). Ambulatory-UDS duration was on average 6 h. The differences in measurements from the recordings for the successful patients are summarized in Table 3. Of the 30 implanted patients, 26 (87%) also showed improvement on ambulatory-UDS. Of all patients who had an unchanged recording, 83% (20/24) failed the test period and were not submitted to permanent implantation. One patient with improvement on ambulatory-UDS during the test period, presented with an acontractile bladder at baseline and the subsequent emergence of some micturition contractions during treatment. However, this patient did not report clinically relevant improvement on voiding diaries. Another patient showed > 50% improvement in the degree and frequency of incontinence episodes, but despite this fact, the patient was not satisfied (enough) with the treatment results. In this patient, improvement during ambulatory-UDS was consistent with improvement in the voiding diaries.
Ambulatory measurements from the baseline and testing period recordings in the successful patients
In 2 of the 4 patients with an unchanged ambulatory-UDS recording, the treatment effect was not reached at the time of the UDS. It was in fact unknown when exactly the treatment effect could be expected, therefore, and for reasons of hospital logistics, the ambulatory-UDS during the SNM test period was scheduled in advance. However, at a later time point, still within the 4 weeks test stimulation period, treatment was proven effective after all and these patients received a definitive implant. In these cases, unfortunately, the ambulatory-UDS was not repeated.
Long-Term Outcome
Patient follow-up was on average 3.2 years (SD 3.8). The 1-year outcome for all 30 implanted patients was favourable. In the 26 patients who displayed improvement on ambulatory-UDS, no decrease in effect was noted during follow-up. Of the 4 implanted patients who did not show improvement on ambulatory-UDS, 2 showed a decrease in effect (but still > 50% improvement) and 2 maintained the same treatment effect at 1-year follow-up.
Discussion
Up and until now, voiding diaries have been used as a gold standard for the assessment of SNM test period treatment outcome. Voiding diaries can be biased due to several reasons. The diaries can be filled out incorrectly or seem to show an improvement at a quick glance, but after correction, for example, for total fluid intake of the patient, will not show any sustained improvement. This study investigated whether in patients undergoing SNM the performance of an ambulatory-UDS could lead to an objective confirmation of success or failure of the treatment. Pressure-flow studies record and measure events real-time; however, they only capture symptoms during one particular and limited time frame. In the ambulatory setting, the study is performed during a longer period of time and with natural filling of the bladder and could therefore have a higher chance of depicting patients’ symptoms compared to a conventional-UDS. Several studies have proven that, in general, voiding diaries recorded by patients are highly accurate, reproducible and more accurate than just the patient’s recollection [16, 17]. However, other studies have shown that in women with urinary incontinence, the correlation between their history and voiding frequency recorded in voiding diaries appeared to be weak [18]. A final statement on the exact value of voiding diaries is yet to be made.
Some have suggested that pressure-flow cystometry mainly gives a qualitative measure of urgency, whereas the voiding diary offers objective and reliable quantitative information of the symptoms and thus supplements the cystometric evaluation. These studies concluded that combining history and voiding diaries was too unreliable and urodynamic testing should not be omitted. Adding data extracted from voiding diaries with other examinations (e.g., voiding diaries, validated symptom score questionnaire, urodynamic studies) may lead to a more adequate diagnosis and consequently, a better treatment response [19-22].
The severity of symptoms as recorded on voiding diaries has no association with the presence of DO [23]. In patients with storage dysfunction, regardless of the presence of DO, additional ambulatory-UDS does not seem to contribute to a better prediction of the success of SNM in the future [15]. In addition, the success of the treatment of idiopathic OAB with onabotulinumtoxinA bladder injections does not appear to be related to the finding of pretreatment DO either [24]. However, DO could be of importance in terms of its effect prediction of other treatments.
The ICS urodynamics committee recommends the use of ambulatory-UDS as a second line diagnostic in specific cases [25]. Our study shows that objective improvement on ambulatory-UDS is associated with the standard evaluation parameters of subjective treatment success and the more objective voiding diary parameters. This shows that the use of ambulatory-UDS are, at least, not inferior to the use of voiding diaries. Furthermore, ambulatory-UDS may help to perform a more objective evaluation of the test stimulation, especially in doubtful cases. Assessment with ambulatory urodynamics may accelerate the decision making process, when we compare this method with more time-consuming voiding diaries. The current standard test period for SNM constitutes 4 weeks; in current study results, we seem to see an earlier onset of effect in changed ambulatory-UDS recordings, than the later moment the symptom improvement becomes obvious. We thus speculate to shorten the test period substantially (±2 weeks), but this should be supported by research developed to investigate this exact statement.
What currently complicates the decision-making process even more is that the exact cut-off value of voiding diary improvement to be used is still a topic of debate. Most experts in the field adhere to the ≥50% improvement, but some have advocated for a ≥70% improvement as a significant effect [26]. Others mention the success and cure rates separately, denominating on the one hand the group of patients with 50% improvement and the other hand the group, which have no symptoms at all after treatment by SNM [27]. It should be noted that current research adhering to the cut-off value of ≥50% improvement, stated that the treatment success outcome measured in incontinence episodes was associated with a clinically meaningful improvement in disease-specific health-related quality of life for those with OAB (with urgency incontinence) [28].
Furthermore, it is hypothesized that urodynamic confirmation of treatment success secures long-term success of treatment as placebo effect can be ruled out. Results from this study are too preliminary to draw such a conclusion. Therefore, a prospective evaluation in a larger cohort is needed. As stated earlier there should also be included the special aim to justify a shorter SNM test -period.
From our results, it can be concluded that ambulatory-UDS can be used to assess the test evaluation in both partial or complete urinary retention and in patients with OAB. A limitation is of course the small number of patients with OAB symptoms in the total study group.
Conclusion
There is a significant correlation between the subjective, voiding diary parameters and results of ambulatory urodynamic studies in patients pre- and post SNM. Hence, an ambulatory UDS can be a useful tool in the selection of successful candidates for permanent SNM therapy. Using ambulatory-UDS to confirm success, instead of voiding diaries, could in the future justify the shortening of the test period.
Acknowledgement
The personnel of the Urology department of the Maastricht University Medical Centre are gratefully acknowledged for their contribution towards this study.
Disclosure Statement
The authors declare that they have no conflict of interest. The local Medical Ethics Committee approved the study protocol. Clinical informed consent was obtained from all patients for the additional ambulatory-UDS.
Author’s contribution
J.D.: Project development, Data collection, Data analysis, Manuscript writing. K.L.J.R.: Project development, Data analysis, Manuscript editing. S.R.: Project development, Data collection, Manuscript editing. T.M.: Project development, Data collection, Manuscript editing. P.K.: Project development, Manuscript editing. G.K.: Project development, Manuscript editing.
References
K.L.J.R. and S.R. contributed equally to the manuscript.

