

Abstract
Purpose: To compare the effect of intravesical interleukin-2 (IL-2) instillations with and without a marker lesion on time to recurrence (TTR) in non-muscle-invasive bladder cancer (NMIBC) patients. Methods: A prospective randomized, controlled trial was conducted. Patients with multiple non-muscle-invasive tumours were randomized for a complete or incomplete transurethral resection (TURBT), followed by 3 IL-2 instillations. The primary end point was TTR. Results: These are the results of an interim analysis, which was performed due to slow accrual after which the study was closed prematurely. Twenty-eight patients were randomized of which 17 were eligible on an intention-to-treat basis. Median TTR or last follow-up was 3 months (interquartile range [IQR] 3–10 months) for the complete and 4 months (IQR 3–8 months) for the incomplete TURBT group. The TTR between the 2 groups did not differ significantly (log-rank, p = 0.54). -Conclusions: These data do not support the hypothesis that a marker lesion enhances the therapeutic effect of IL-2 instillations in patients with NMIBC.
Introduction
The initial management of non-muscle-invasive bladder cancer (NMIBC) consists of transurethral resection of the tumour (TURBT) followed by intravesical chemotherapeutic or Bacillus Calmette-Guérin (BCG) instillations depending on the European Association of Urology risk group assignment [1]. Chemotherapeutic instillations are known to reduce recurrence rates, but do not reduce the risk of progression [2]. BCG-instillations are more effective in reducing recurrence rates and do reduce the risk of progression [3, 4]. The precise mechanisms of the therapeutic effect of BCG-instillations are not yet fully understood, but it is believed that a local immune reaction plays an important role [5]. The major drawback of BCG is its toxicity: side effects of BCG are more frequent and more severe as compared to those of chemotherapy [3]. Furthermore, despite the beneficial effect of chemotherapeutic and BCG-instillations, the risk of recurrence remains high ranging from 31 to 78% [6]. Hence, there is an unmet need for a more effective and less toxic treatment. Given the successful oncological results after treatment with BCG-instillations, there is interest in other immunotherapeutic agents.
Interleukin-2 (IL-2) has been used to treat several kinds of cancers [7, 8]. Intravesical instillation of IL-2 seems of interest for treating BC patients, since patients who respond to BCG-instillations have higher urinary levels of IL-2 [9-11]. Furthermore, several reports have demonstrated a therapeutic effect after intralesional treatment [12], intravesical instillations [13, 14] and continuous intravesical perfusion [15] with IL-2 in BC patients. Previously, our group compared 2 studies in which the effect of intravesical IL-2 instillations on the risk of recurrence in NMIBC patients was assessed [16]. In one study, 0.5–1.0 cm of tumour was left intact at TURBT as a “marker-lesion” [17], whereas in the other study, all patients were treated with complete resection [18]. Comparison of these 2 studies suggested that IL-2 is more effective in case a marker-lesion is left behind [16]. These findings form the basis for the hypothesis that IL-2 needs tumour associated antigens to initiate an immune reaction (which are gone after complete resection). We performed a randomized clinical trial that evaluated the effect of intravesical IL-2 instillations in patients with NMIBC who either underwent a complete or an incomplete TURBT.
Patients and Methods
Study Design
A prospective, randomized controlled study was conducted in the VU University Medical Centre (VUmc), Academic Medical Centre, Catharina hospital, and Medical Centre Alkmaar between June 2012 and November 2017. The institutional review board (VUmc) approved the study (2010/295). Written informed consent was obtained from all patients. This trial was registered in a public trials registry (EudraCT 2010-020397-42).
Patients were randomized for a complete or incomplete TURBT (marker-lesion group) followed by IL-2 instillations.
Inclusion and Exclusion Criteria
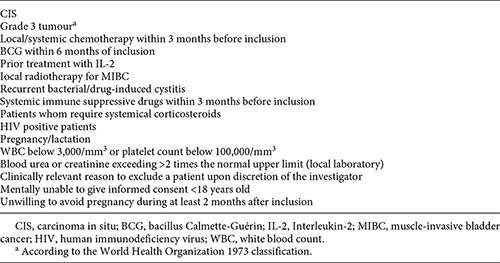
Patients with multiple (< 10) Ta G1–2 (WHO 1973) [19] bladder tumours of which one was 5–10 mm were eligible. Patients with grade 3 tumours or CIS were excluded. Other exclusion criteria are listed in Table 1. Some patients were expected to be excluded after randomization, based on histopathological evaluation.
Randomization and Treatment
A computer-generated random number table was created and used by the study coordinator to allocate patients to the complete TURBT or marker-lesion group. A 1: 1 allocation ratio was used and allocation occurred at the central research office at the time of enrolment. The patient was blinded for the allocation, until TURBT. All visible tumours were completely removed by TURBT, except for one marker-lesion (5–10 mm) in the marker-lesion group. The marker-lesion always was a separate tumour and the size of the marker-lesion was estimated using the size of the resection loop as reference. Within 24 h after TURBT, an instillation containing 6 × 106 units of IL-2 (Proleukin®, Novartis, Amsterdam, the Netherlands) dissolved in 50 mL of 0.9% saline plus 0.1% Human Serum Albumin was instilled into the bladder via a transurethral catheter. The solution remained in the bladder for 1 h, after which the catheter was removed. At days 7 and 14 after TURBT, another IL-2 instillation was administered in the same manner at the outpatient clinic. Patients were instructed not to void for 1 h.
Follow-up
Patients were followed with cystoscopy with a 3-month interval for the first 2 years after initial TURBT and every 6–12 months thereafter in case of no recurrence. TURBT was performed in case of a remaining marker-lesion at 3-months cystoscopic follow-up or if there was a suspicion for recurrence at any time. In case of a recurrence or a persistent marker-lesion, patients were withdrawn from the study and standard care was applied. If histological evaluation after the initial TURBT showed inappropriate tumour characteristics (e.g., Grade 3/CIS; Table 1), patients were also withdrawn from the study and standard care was applied.
Endpoints
The primary endpoint was time to recurrence (TTR). Recurrence was defined as a lesion in the bladder confirmed by histological evaluation after second TURBT. If a TURBT could not be performed (e.g., due to death prior to second TURBT), a suspicious lesion at cystoscopy was also considered a recurrence. Secondary endpoints were the percentage of completely regressed marker-lesions on cystoscopic follow-up 3 months after first TURBT, the incidence of adverse events (AE) and the quality of life (QoL) at 3, 12, and 24 months after TURBT as compared to QoL at screening (section QoL and AE).
QoL and AE
Two questionnaires were administered to determine the QoL: the Short Form 36 (SF-36, Dutch version) and the QoL Questionnaire for Superficial Bladder carcinoma (QLQ-BLS24) [20-23]. The SF-36 is a general QoL questionnaire; the QLQ-BLS24 is used to measure BC specific QoL. Individual and scale item scores were transformed into scores ranging from 0 to 100. Both questionnaires were taken at the time of inclusion and at 3 months after first TURBT. All AE reported by the patient or observed by the medical personnel/investigator were recorded.
Sample Size
A power calculation was performed, in PASS 12 software (NCSS, LLC, Kaysville, UT, USA) using the Mann-Whitney Wilcoxon test procedure, based on the assumption that the TTR was exponentially distributed. The mean TTR for the complete and incomplete TURBT-group was set at 5 and 15 months respectively. To detect this difference at error rates of α = 0.05 and β = 0.10, with an estimated 20% violation of inclusion criteria, a total of 33 patients was needed in each study arm.
Statistics
Continuous data were summarised with mean and standard deviation. Categorical data were presented with frequencies and percentages. The χ2-test was used to compare categorical data between groups, the independent samples t test was used to compare means of continuous data between groups. Kaplan-Meier curves were constructed for each study arm and compared with the log-rank test. Patients lost to follow-up without an event of interest were censored at the last date of follow-up. Intention-to-treat analysis was performed for all eligible randomised patients, including patients with a protocol violation (CONSORT statement) [24]. Excluded patients that did receive at least one instillation of IL-2, were included in the analysis of AE. Differences in scores of QoL-scales before and after treatment (Δ-scores) were calculated and compared using the Mann-Whitney U test. Crohnbach’s α coefficient was calculated to assess the consistency of the items in the BLS-24.
All analyses were performed with SPSS software (SPSS 22.0, IBM, Armonk, NY, USA). All tests were two-sided and a significance level of 0.05 was applied.
Results
Patients
Because of slow patient accrual, an interim analysis was performed. The trial was closed prematurely on November 1, 2017 after consulting the medical Ethical Committee.
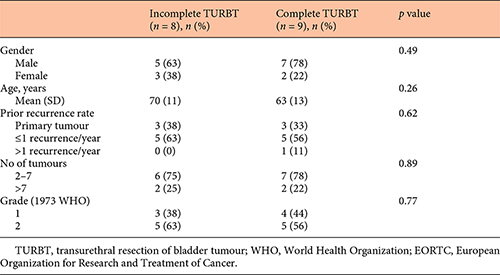
Between May 2012 and May 2017, 28 patients were randomized in 4 hospitals in the Netherlands: VU University Medical Center (n = 21), Medical Center Alkmaar (n = 2), Academic Medical Center (n = 3) and the Catharina Hospital (n = 2). After randomization, 11 out of 28 patients were excluded (Fig. 1), mostly because of unfavourable histology (9/11 excluded patients). Two tumours were not considered suitable to serve as a marker-lesion at TURBT; in one patient, there was no lesion of 0.5–1.0 cm (all tumours were larger). In the other patient, the tumours were too close to each other to perform an incomplete resection without damaging the vascularization of the marker-lesion. Eventually, 17 patients were included in the analysis. Baseline characteristics were similar between the 2 treatment groups (Table 2).

Primary Endpoint (TTR)
The median follow-up was 13 months (interquartile range [IQR] 3–13) for patients without a recurrence. After total follow-up, 14 out of 17 patients developed a recurrence (n = 7 complete and n = 7 incomplete TURBT group). Multiple recurrences were diagnosed in 5 patients (n = 2 complete and n = 3 incomplete TURBT). Median TTR or last follow-up was 3 months (IQR 3–10) and 4 months (IQR 3–8 months) for the complete and incomplete TURBT group respectively. The difference in TTR between the incomplete and complete TURBT group was not statistically significant (log-rank, p = 0.54; Fig. 2).

Kaplan-Meier curve of time to recurrence (TTR) or persistent marker-lesion for patients treated with an incomplete transurethral resection or a complete transurethral resection.
Kaplan-Meier curve of time to recurrence (TTR) or persistent marker-lesion for patients treated with an incomplete transurethral resection or a complete transurethral resection.
Secondary Endpoints
Marker-Lesion Regression
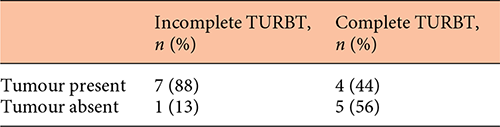
At 3-months cystoscopy the marker-lesion dissapeared in 1 out of 8 patients and that patient remained recurrence-free after 13 months of follow-up (Table 3). In one patient, the marker lesion increased in size while the lesion became smaller in another patient. In the latter patient follow-up TURBT was refused. After 7 months the marker-lesion disappeared without further intervention. The patient remained recurrence-free after 11 months of follow-up. In the 5 remaining patients the lesion remained of similar size as at initial TURBT.
In 2 other patients, the persistent marker-lesion was not confirmed by histological evaluation. One patient died of de novo metastasized non-small cell lung cancer before second TURBT could be performed. The other patient initially refused treatment of the marker lesion but agreed to TURBT after 7 months of follow-up. Histological evaluation confirmed a pTaG2 tumour.
In the complete TURBT group, 4 out of 9 patients had a recurrence at 3-months cystoscopy.
Quality of Life
The QoL questionnaires (SF-36 and BLS-24) were completed at baseline as well as at 3 months follow-up in 14 out of 17 patients (complete TURBT n = 7, incomplete TURBT n = 7). None of the Δ-scores differed significantly between groups (online suppl. Table 1, 2, see www.karger.com/doi/10.1159/000493159). The number of completed questionnaires after 3 months of follow-up was too small to make any comparisons.
Adverse Events
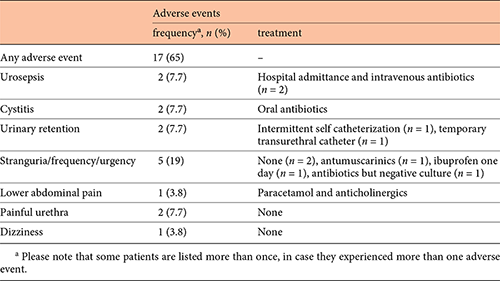
A total of 26/28 patients received at least one instillation of IL-2, of whom 17 out of 26 (65%) patients experienced at least one adverse event (complete TURBT n = 8, incomplete TURBT n = 9, p = 0.4). A full list of AE is presented in Table 4. Two serious AE occurred; both patients developed a urinary retention postoperatively that was treated with a transurethral catheter, followed by urosepsis after catheter removal.
Discussion
In this study, we aimed to determine the role of an antigenic marker-lesion in the efficacy of IL-2 instillations in patients with NMIBC. To our knowledge, this is the first study that analyzed the role of a marker-lesion when applying IL-2 instillations in a prospective, randomized, multicentre setting. Further strengths include the well-documented AE.
Our initial hypothesis was that the presence of a marker-lesion would improve the therapeutic effect of IL-2 due to the presence of tumour associated antigens. The presence of these antigens would boost the host immune response and, similar as seen in BCG, would reduce the risk of recurrence. Yet, after 3 months of follow-up, the marker-lesion regressed in only one out of 8 patients (13%) in the marker-lesion group. After an interim analysis, of which the results led to the premature closure of the study, no statistically significant difference was demonstrated in TTR between the complete TURBT group and marker-lesion group.
Our results do not concur with those from a previous pilot study in which the marker-lesion disappeared in 8 out of 10 (80%) patients after 2 months follow-up [17]. A possible explanation for this discrepancy could be found in the definition of a marker-lesion. In the pilot study, 0.5–1.0 cm of a tumour (partial resection) was left intact, whereas in the current trial, an individual marker-lesion was left intact. In case of incomplete resection of a tumour, damage to the vascularisation of the remaining part of the tumour cannot be excluded. Hence, the regression of the tumour in the pilot study could be caused by damage to the remaining tumour instead of by the IL-2 instillations. Another explanation could be that 3 instillations were used in the current study as opposed to 5 in the pilot study.
In 1 patient, the marker-lesion reduced in size and eventually disappeared without intervention, suggesting that in some patients, more time is needed to obtain a therapeutic effect.
The number of patients with a recurrence at 3 months was high, in both the incomplete (7/8, 88%) and complete resection groups (5/9, 56%). This raises the question whether patients treated with a complete TURBT truly had a recurrence or that residual tumour was present. Eighty per cent (4/5, complete resection group) did have a recurrence at the resection site. However, 3 patients had multiple tumours at other locations in the bladder as well, suggesting that the urothelium of these patients is prone to malignant transformation as opposed to residual tumour as the result of an incomplete resection (alone). The high recurrence rates in both groups also raise doubts about the efficacy of IL-2 instillations in general, with or without a marker lesion.
In contrast to the literature on intravesical instillations with IL-2 [13, 14, 17, 25, 26], the number of AE in this study was high (17/26, 65%). However, most AE are known complications after TURBT and most likely not caused by the IL-2 instillations.
A major concern is that this study closed prematurely and thus is underpowered. The compliance was lower and the accrual slower than expected beforehand. The low compliance was mainly caused by unsuitable histology after TURBT (Fig. 1). These exclusions are inherent to the study design, as histological evaluation becomes available only after randomization. The exclusion rate was however higher than expected beforehand (61 vs. 80%). Reasons for slow accrual include the overestimation of the number of patients with multiple resectable tumours, as well as patients’ refusal to participate in the study due to the possibility of an extra surgical intervention (TURBT of the marker-lesion).
The treatment protocol in the current study differs from the schedule used in the pilot study. In the pilot study, 5 instillations were administered for 2 h on 5 consecutive days [17]. In the current study, 3 instillations were administered for 1 h within 24 h and 7 and 14 days after TURBT. Whether better results would be obtained in case of a different schedule cannot be answered from our data.
In future studies, it would be interesting to study the effect of preoperative intratumoral IL-2 [12]. Intralesional application might overcome the problems with accrual, since there is no risk of a second TURBT for a persistent marker-lesion. Furthermore, patients with single tumours would be eligible and the therapeutic effect could be measured from reduction in tumour size measured at the diagnostic cystoscopy and the cystoscopy at TURBT.
Conclusions
Our findings do not support the hypothesis that a marker lesion enhances the therapeutic effect of IL-2 instillations in patients with NMIBC. The high recurrence risk in both treatment groups raises a doubt whether 3 IL-2 instillations, as a monotherapy, reduce the risk of recurrence in patients with NMIBC.
Acknowledgements
We thank Innovatiefonds Zorgverzekeraars, which provided a research grant to financially support our study. We thank Novartis for providing us IL-2 instillations. The funder did not have a role in the study design, collection analysis and interpretation of the data nor in the writing of the report or the decision for submission. Furthermore, we would like to show our gratitude to all centres for participating in this study, particularly to Dr. T.M. de Reijke, Dr. E Koldewijn, Dr. S. Bos and Dr. M. Kuehen. Finally, we thank Jannette Bossenga for her assistance in the trial coordination.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
The authors declare that they have no conflicts of interest to disclose.
Funding Source
This study was funded by Innovatiefonds zorgverzekeraars. IL-2 was provided by Novartis.
References
J.A.N. and A.H. authors contributed equally.

